What is CPAP and how does CPAP work?
CPAP treatment Continuous positive airway pressure therapy (CPAP) uses a machine to help a person who has obstructive sleep apnea (OSA) breathe more easily during sleep.
A CPAP machine increases air pressure in your throat so that your airway does not collapse when you breathe in.
There is no difference in treatment success between both types of machines (CPAP and APAP). The APAP machines are generally more expensive than CPAP. Paying the extra cost for an APAP machine is generally not needed or recommended except in some selected cases.
Types of CPAP masks:
The CPAP machine will have one of the following attached to it:- A mask that covers your nose and mouth known as a full face CPAP mask
- A mask that covers your nose only-called a nasal CPAP mask
- A mask that fits directly into the base of your nose, with pillow type cushions that seal around your nostrils, known as a nasal pillows CPAP mask
Types of CPAP machines:
There are 2 types of CPAP machines, ones that offer fixed air pressure and ones that offer automatically adjusted air pressure, often known as Auto or APAP machines.How Does CPAP Work?
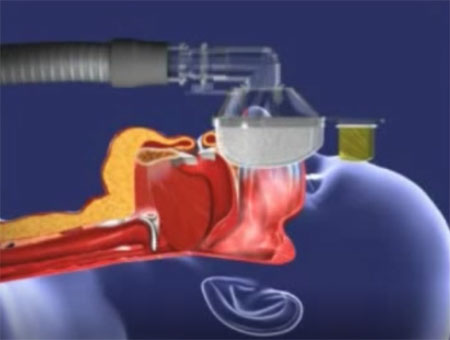
To understand how a CPAP machine works, you should know how obstructive sleep apnea works. Obstructive sleep apnea occurs when the throat muscles and tongue collapse into the airways during sleep, blocking airflow. This airway blockage sends a message to the brain that the body needs to breathe, awakening it from sleep to take a loud, gasping breath. Individuals with mild obstructive sleep apnea experience 5-15 of these episodes per hour of sleep, while individuals with severe obstructive sleep apnea experience more than 30. A CPAP machine works by continuously blowing gentle, pressurized air through the airway. The increased air pressure prevents the airway from collapsing when you breathe. CPAP Machine Effectiveness When used as directed, CPAP therapy can immediately improve the quality of life for individuals who suffer from obstructive sleep apnea. You’ll likely notice less snoring, fewer breathing obstructions and a decrease in daytime sleepiness—among other health benefits. Research has shown that using a CPAP machine can reduce the risk of health problems linked with obstructive sleep apnea, such as high blood pressure, depression and cardiovascular issues.Difficulties with CPAP
Problems that may occur with CPAP include:- Dry nose and sore throat.
- Nightmares and excessive dreaming during early use.
- Nasal congestion, runny nose, and sneezing.
- Irritation of the eyes and the skin on the face.
- Abdominal bloating.
- Leaks around the mask because it does not fit properly.